

Abstract
Introduction:
MPN-related pain, including abdominal discomfort (53.2%), and bone pain (48.5%), is a prevalent complaint within the disorder and is associated with impaired patient quality of life, reduction in most functional domains and overall poor prognosis. Non-targeted treatments for MPN disorders have been previously shown to provide little symptomatic relief for MPN pain. To date, little is known about patient viewpoints on MPN pain, its relationship to other chronic pain syndromes and the impact of pharmacologic and non-pharmacologic pain therapies. In this study, we performed an international survey of MPN patients to better understand the prevalence and management of MPN pain.
Methods:
This study was performed by the MPN Quality of Life Study Group. A survey was designed by a team of MPN investigators experienced with MPN symptomatology. Survey content included the Barriers Questionnaire II (BQII), a 27-item survey validated to assess patient belief barriers to optimal management of cancer pain measured on a 0 (do not agree at all) to 5 (agree very much) scale (Pain. 2002 Oct;99(3):385-96.). Patients also completed the MPN-10, a 10-item survey of MPN symptoms completed on a 0 (absent) to 10 (worst imaginable) scale (Blood. 2011 Jul 14;118(2):401-8). The survey was posted on high-traffic MPN-related webpages focused on patient education and advocacy (MPN Forum, MPN Net, MPN Research Foundation, MPN Voice) for a total of 28 days. Survey questions evaluated patient demographics, pain histories, current and prior treatment strategies, as well as satisfaction with and barriers to available treatment options.
Results:
Demographics
A total of 502 MPN patients (MF 26.9%, PV 44.2%, ET 28.9%) completed the survey. Patients were of expected mean age (60.5 years) and primarily female (74.9%). Most were from the United States (66.7%) and primarily English speaking (92.2%). Patients described being diagnosed with their MPN 3 to 10 years (35.4%) or >10 years ago (30.8%). Splenic enlargement was vocalized by 36.5% of patients and few patients had had a known history of blood clots (25.4%), severe bleeding (13.3%), conversion to acute leukemia (0.4%) or prior bone marrow transplant (1.4%). Patients described a treatment history of a variety of MPN therapies including aspirin (82.7%), hydroxyurea (60.6%), phlebotomy (40.6%), ruxolitinib (25.9%), interferon (18.5%), anagrelide (17.3%), active clinical trial (5.0%) and radiation treatment (0.4%).
Pain Severity, Prevalence and Treatments
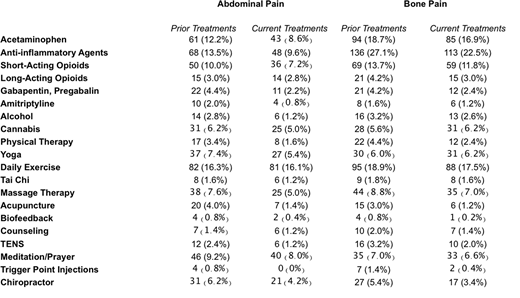
Among surveyed patients, the MPN-10 mean was 28.3. Mean individual symptom scores and prevalence were 3.1 and 65.6% for abdominal discomfort and 3.0 and 60.4% for bone pain, respectively indicating a low to moderate symptom burden. Most patients had no prior history of chronic pain prior to their MPN diagnosis (47.1%), with chronic abdominal pain and chronic bone/muscle pain noted prior to MPN development in 5.6% and 20.8% of patients, respectively. Most patients felt that their chronic pain has either stayed the same (26.2%), worsened (28.3%) or significantly worsened (14.5%) since their MPN diagnosis. Many patients found pharmacologic and non-pharmacological therapies efficacious for individual pain symptoms, and 42.1% described regularly taking medication to control their pain (Table 1).
Barriers to Pain Management
Overall, 42.3% of MPN patients reported being unsatisfied with their current pain management plan. Despite this, only 43.5% of patients stated that their MPN providers discussed pain during office visits. Palliative Care (3.1%) and Pain Management (7.3%) were infrequently engaged. On the BQII, patients described being confident that cancer can cause pain (mean 4.2, SD 1.1) but did not necessarily expect to have pain following their MPN diagnosis (mean 2.2, SD 1.8).
Conclusion
Chronic pain (abdominal, bone) is a prevalent and undermanaged feature of MPN disorders. Chronic non-MPN pain is further complicated by the development of the disorder. Many MPN patients lack understanding on its prevalence and furthermore feel ill-equipped to manage it. Patients have, however, found symptomatic benefit from various pharmacological and non-pharmacological treatment modalities that require further exploration. Results from this study suggest MPN patients should be assessed regularly for pain and offered early referral to specialized services for evaluation, source identification and treatment.
Scherber:Incyte: Consultancy; Orphan Pharmaceuticals: Honoraria. Mesa:Ariad: Consultancy; Galena: Consultancy; CTI: Research Funding; Incyte: Research Funding; Promedior: Research Funding; Gilead: Research Funding; Novartis: Consultancy; Celgene: Research Funding. Dueck:Bayer: Employment; Pfizer: Honoraria; Phytogine: Employment. Palmer:Novartis: Research Funding.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal